Medicare: Australians face steeper health costs as prevention funding lags


Raising the bulk billing rate will not solve a culture primarily profit-driven. Photo: Getty
You might have noticed your last medical bill was higher than usual.
Whether it’s a GP visit, getting a test, or seeing a psychologist, Australians are paying more for healthcare as Medicare struggles with the rise in chronic disease and mental health care.
The threat is so great that doctors last week warned the affordability of Australia’s “world class” health system was at risk as longer, more complex appointments drove up patients’ out-of-pocket costs.
“Government has only taken the first steps to rebuild Medicare and general practice after decades of under funding and the Medicare freeze,” Royal Australian College of General Practitioners boss Nicole Higgins said.
But while GPs want billions more in federal funding for Medicare rebates, other experts say curbing higher costs for patients and taxpayers will require much broader reform.
Grattan Institute health program director Peter Breadon warned Australia remained “well behind” other countries in spending on prevention policies that could stem the rise of chronic disease.
That included taxes on sugary drinks that were already in force in Britain, France and Finland, Breadon said, as well as globally lax restrictions on companies advertising unhealthy foods.
“If we don’t take those steps now, we will be paying the price in 10, 15 or 20 years’ time,” he said.
“It’s critical to get the best return on that [public] investment, and that means less just putting out un targeted subsidies and more focusing resources where they’re most needed.”
Modernising Medicare
Medicare celebrated its 40th birthday in February, and while Australia’s public healthcare system is considered among the best in the world, it has also rapidly fallen behind and needs reform.
University of Technology Sydney distinguished professor in health economics Jane Hall said pressures on affordability were growing as Australia’s medical problems changed.
“We’ve always relied on some form of out-of-pocket costs to keep the system in some sort of balance,” Hall said.
“As a society, we’re going to need to pay more for healthcare; it’s getting more expensive dealing with chronic disease and complex [mental health] problems in younger populations.”
Earlier this year the federal government published a landmark review that mapped out a plan to modernise the public health system, focusing on new funding models and higher quality care.
It led to a trial of what’s called blended funding, where doctors are given a flexible care budget tied to a patient, in addition to some subsidised fee-for-service payments, for each appointment.
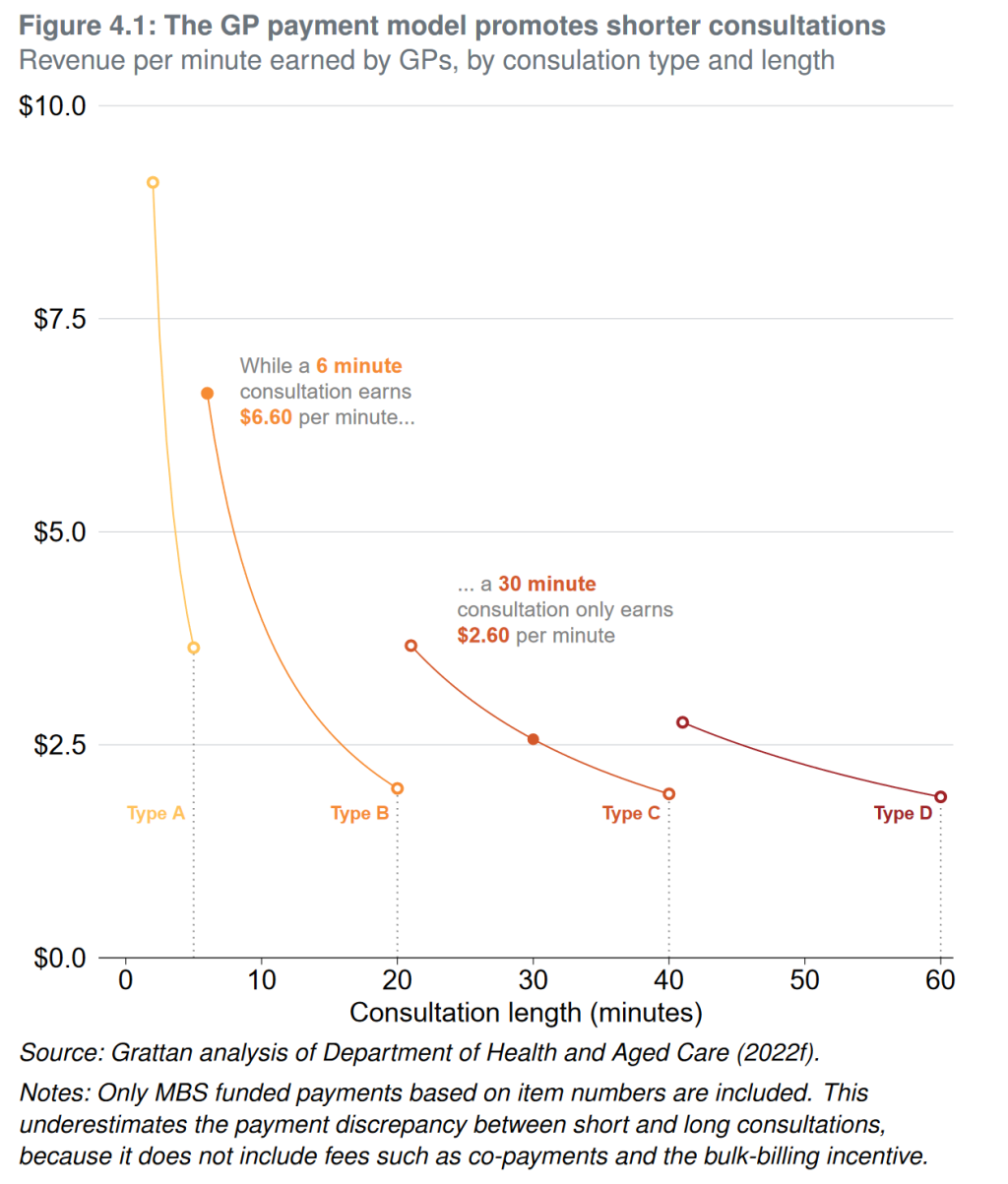
The idea is that GPs will be better compensated for more complex care than under Medicare’s current model, which simply pays them for each service provided, incentivising shorter visits.
“[Medicare] was developed back in the days when more health conditions were addressed by one-off visits – with chronic disease, you’re supporting people managing it over decades,” Breadon said.
“Many other countries have brought in blended funding models.”
Doctors groups have backed the changes, but have argued they don’t go far enough to lift rates of funding and that a further 20 per cent increase in rebates for GP consultations is still required.
Their latest survey this week showed mental health demand among younger Australians is driving recent rises in out-of-pocket costs, underscoring how complex care is straining Medicare.
But UTS associate professor Nathan Kettlewell said higher rebates wouldn’t solve the problem and could instead direct funds to an area where patients wouldn’t see the biggest benefits.
“Increasing Medicare rebates is in some sense a Band-Aid and it’s quite a costly one,” he said.
“We need to be thinking about more targeted ways to get at the funding gaps without leaking taxpayer money to boost the incomes of GPs without changing the benefits for patients.”
Kettlewell agreed that governments would need to focus more on prevention in coming decades to curb rising costs for both patients and taxpayers.
Source: Grattan Institute
Australia behind on prevention
Australia has a somewhat mixed record with public health prevention policies, having had broad success with campaigns to reduce smoking in recent decades, and now also around vaping.
But elsewhere there are no taxes on sugary drinks, despite decades of loud advocacy from health experts, and companies can quite freely advertise their junk (ultraprocessed) foods.
Breadon said prevention was also a smaller part of Australia’s health budget than in other countries.
While Australia’s per capita health spending was higher than the OECD average in 2018-19, research shows preventative health was only 1.34 per cent of the budget, compared to an average of 2.8 per cent across the OECD.
“The Commonwealth government has an election commitment to establish a centre for disease control,” Breadon said.
“We haven’t seen what that model will look like, but we’d like to see a really strong, independent CDC that can make clear advice to governments about the [prevention] policies that are needed.”
Hall said, however, the adage that prevention is cheaper than a cure can be “misguided”, with a lack of consistent evidence about where increases in taxpayer funding should actually be directed.
“It all sounds very nice but we don’t have the evidence to support it,” she said.
“Whenever you look at these programs you get some that will give you a good pay-off and others that just add to cost.”
The scope of prevention spending could even extend outside of health policy, Hall said.
“One of the things we do know is that early childhood education is one of the best investments,” she said.
“You pick up issues early and get them on a better educational path, which makes them better at managing their health.”
Want to see more stories from The New Daily in your Google search results?
- Click here to set The New Daily as a preferred source.
- Tick the box next to "The New Daily". That's it.

Reasons to be hopeful amid economic gloom

Jobless fall leaves door open to more rate hikes


The billionaire who failed Whyalla steelworks

Carveouts for business after budget backlash



